
A Family History
{kind=link}
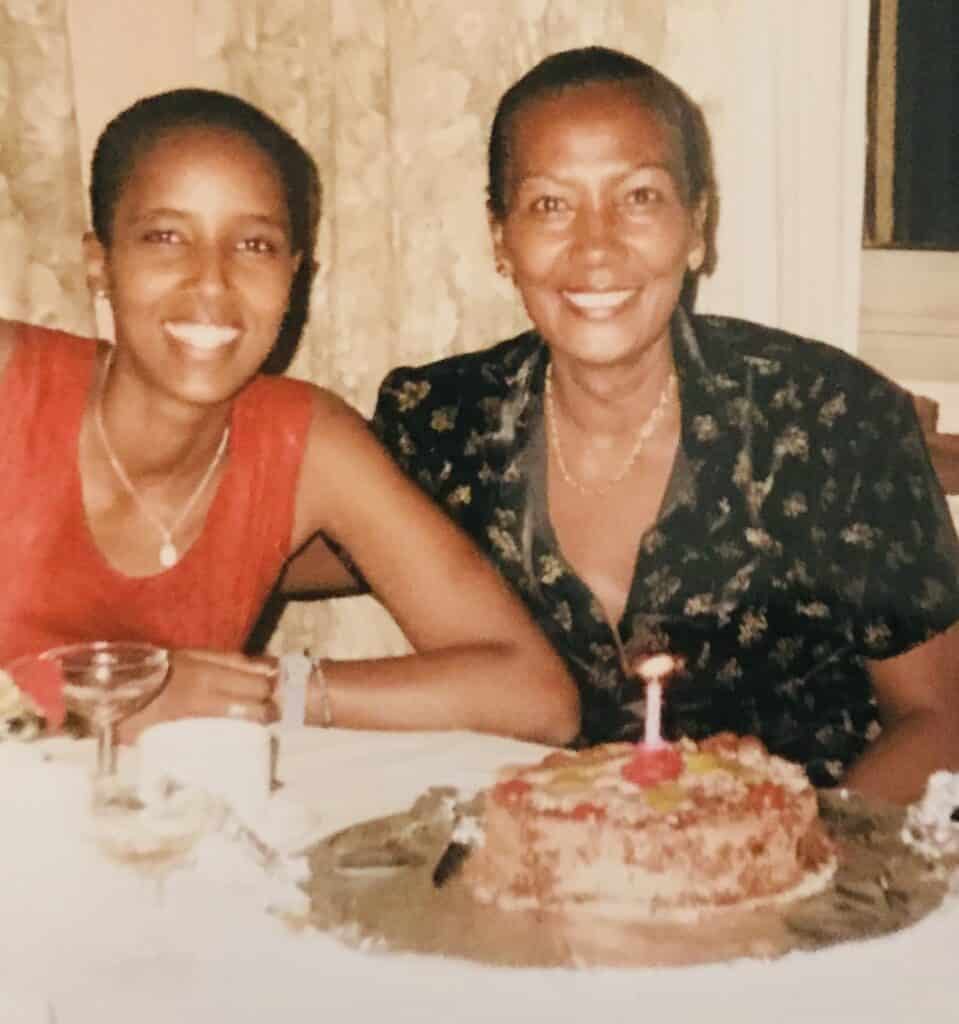
I was 37 years old when my mom died. Together, we shared a lifetime of experiences: birthdays, trips, and graduations. But now, a decade after her death, the two events that linger most vividly in my mind are the moment I watched her take her last breath and the day I found out that her mom – my grandmother – had died of the same disease she had just been diagnosed with and would eventually kill her.
My mom disclosed diagnosis to me breezily, in a quick phone call as she got ready to travel for surgery. “They say I have cancer,” she announced. She was on her way to Thailand, a place some of her friends and colleagues had traveled from Ethiopia to access medical care that was unavailable at home. “Thailand! Isn’t that great?” She tried, unsuccessfully, to make it sound like it was a fun exotic holiday.
Within a few weeks, I discovered that she had ignored symptoms for years and was now living with Stage IV cervical cancer. I asked her to join me in Johannesburg, where I had found a doctor who could provide her with follow-up treatment closer to home. It was a warm and sunny November day. While the gynecologic oncologist examined my mom behind a curtain, I looked out the large windows at jacaranda trees showing off their last flowers of the season. I heard the snap of the latex gloves, as the doctor told my mom to take her time getting dressed. She sat down to face me at her large wooden desk, beginning to jot down notes. “Is there a history of cancer in your family?” she asked. I had always shrugged, embarrassed at this question. Personal health was not a topic my people discussed. But this was a relevant question because along with multiple pregnancies, smoking, certain sexually transmitted infections, and obesity, family history was a risk factor. My mom was still getting herself together on the other side of the large sun-dappled office. I could not see her, but I heard her shuffling slowly.
“Hey mom,” I said, loud enough for my voice to carry. “Is there a history of cancer in the family?”
“Yes.“ She paused “My mother died of cancer.”
It was my first time hearing this. The doctor held her pen up above her chart.
“Oh?” I followed up. “What kind?”
Another pause. Longer this time.
“Cervical.”
Her words hung in the room, floating on the shadows of the tree branches that danced around the walls. I turned my head slowly towards the doctor. She leaned towards me and whispered, “When was your last pap test?”
According to the World Health Organization (WHO), cervical cancer is the fourth most common cancer among women globally. Of the 20 countries with the greatest incidence of the disease, 19 are in Africa. This burden is attributed to the lack of screening, difficulties in accessing treatment, and the comparatively high prevalence of HIV (which is a risk factor). [1] And in the United States, possibly for many of the same reasons, Black women experience a higher mortality from cervical cancer than any other ethnic group.
If diagnosed early, cervical cancer is highly treatable. But my mom, like so many other women, accessed care late. Within 18 months of the medical exam in that sunny room – despite surgery, chemotherapy, and radiation – she had succumbed to the disease, joining the unimaginably long list of women who die of cervical cancer every two minutes. I was stunned by this WHO statistic. Every 120 seconds, a mother, auntie, friend, sister, colleague, and daughter dies of an entirely preventable and treatable disease.
In conversations with my mom and her doctors while she was getting treated, I found out that despite her relatively good access to information and healthcare, she had never had a pap test (also known as pap smear) – the screening for signs of cervical cancer. This screening is recommended to all women when they turn 21, and regularly thereafter. The cervix connects the uterus and the vagina, and the pap test – which assesses whether there are changes or abnormal cells in the cervix – requires a pelvic exam, which some women find unpleasant. Of course, this type of preventive care is not a given for many women in low- and middle-income countries, or in marginalized and uninsured communities in the United States. And once symptoms begin – vaginal discharge, abnormal bleeding, vaginal odor – many women delay seeking help despite discomfort and pain. Ten years later, it still breaks my heart to think of my mom suffering self-consciously through her symptoms and simply hoping for the best.
The doctors had told us that they would do all they could, but that starting treatment at Stage IV made the likelihood of survival less likely. My mom had always joked that she wanted to live for a whole century, but there she was on her death bed at 70 – eerily the same exact age her own mother was when she died. As with the thousands of women who died of cervical cancer that year in Ethiopia, my mom’s cause of death was listed as cancer. But the truth is that as much as they are being killed by the disease, women are also being killed by an abundance of shame and stigma regarding their reproductive health and a lack of access to quality care. In my mom’s case, she was on a tragic path laid by her own mother, decades prior.
In 2020 (the most recent year for which WHO has released global data), 342,000 women – mostly African and of African descent – died of cervical cancer. I can’t help but imagine their daughters and nieces watching these women slip away and wondering – as I did – what they could have done differently.
Every January, the WHO marks Cervical Cancer Awareness month. According to their website, they aim to eliminate the disease by the end of the century by promoting the tools that are available to achieve this goal: screening, treatment, and the roll-out of the Human Papillomavirus (HPV) vaccine. Data shows that the vast majority of cervical cancer cases are caused by HPV, which is one of the most widespread sexually transmitted infections worldwide. According to the US Centers for Disease Control and Prevention, “HPV is so common that nearly all sexually active men and women get the virus at some point in their lives.” Thankfully, the world now has access to an effective vaccine that can help protect women from infection, especially when it is accessed early in life (preferably before age 26).
Given my family's risk of cervical cancer, I received the HPV vaccine in my late 30s. I am an enthusiastic advocate for the rollout of all effective and safe medical tools. But what my years of public health experience and family losses have taught me is that if we don’t tackle shame, stigma, and lack of information with the same energy we use to roll out those tests, treatments, and vaccines, we risk failing miserably.
We must refuse to allow that to happen. The ability to alter family history lies in our hands.